

Cancer survival has been steadily improving in most cancers for many years and we can help this trend continue in two broad ways.
Firstly we can improve the stage at which a cancer is diagnosed (the earlier the better) through earlier diagnosis initiatives.
Or secondly we can improve the survival at specific stages at diagnosis by changing patterns of care or introducing new clinical techniques or technologies.
To differentiate between improvements due to these two factors we need to understand in detail, and separately for each cancer type, the proportion of tumours diagnosed at each stage, and how survival varies with stage.
We have published a new report on cancer and survival that examines this.
Stage at diagnosis and cancer survival
One of the main factors for poor chances of survival from cancer is the stage of the tumour at diagnosis.
Small, localised, stage 1, tumours are far more curable, while the treatments available for stage 4 tumours that have spread to distant sites around the body are much harder to cure and treatments are usually intended to reduce suffering and improve quality of life.
Between these extremes are stage 2 and 3 where the tumour has increasingly spread through the body (the exact classification varies with the type of cancer) and curative treatment may be more or less possible.
Using improving cancer registration data
The proportion of all cancers in England with a known stage at diagnosis has leapt upward and now stands at 77% for all malignant cancers combined (excluding non-melanoma skin cancer).
For the ten major cancers reported in the Public Health Outcome Framework it is even higher at 88%.
Cancer registration has been integrated at a national level for all cancer cases diagnosed in England since January 2012, and stage information has been improved by closer working with frontline services, improved collection of radiological data and standardised national processes.
So we now have three years of data for many cancers, shown below, where both the stage breakdown and the net survival are well recorded (net survival is the survival after allowing for mortality due to causes other than cancer).
Overall survival for all stages combined has increased in some cancers (including lung, kidney, and ovarian) by over 10% in the last ten years.
Previously we have struggled to understand whether these increases represent genuine success in earlier diagnosis, real change in stage specific clinical outcomes or other factors.
The problem with lung cancer and variation by cancer type
There is substantial variation across different cancer types in the proportion of cancers diagnosed at each stage. For breast and uterine cancers, and melanomas, more than three quarters of tumours are diagnosed at early stage (that is, stage 1 or 2).
For lung cancer though, three quarters are diagnosed at late stage (stage 3, 4 or Unknown), while for prostate, colorectal and ovarian cancer over half are diagnosed at late or unknown stage.
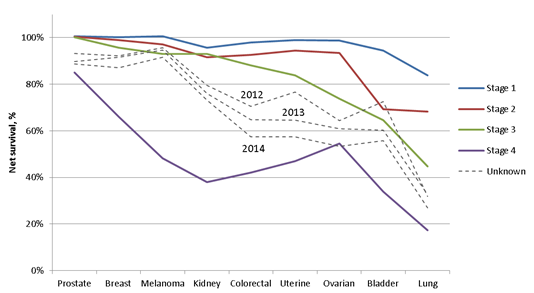
Survival also varies strongly with stage in different cancer types, as shown below.
For five cancer types one-year survival is over 85% even in stage 3 cancer, while in the others (uterine, ovarian, bladder, and lung cancers) the reduction in survival with increasing stage at diagnosis becomes increasingly steep.
These patterns inform us where progress could be made in improving one year survival and whether we should focus on earlier diagnosis, better stage specific treatment, or both.
In lung cancer, for example, any shift to earlier stage of diagnosis will bring survival benefits and so will any improvement in stage-specific survival.
Of course this data only covers one-year survival, but as we continue to collect high quality stage data we will be able to progressively follow-up survival by stage to five-years and longer.
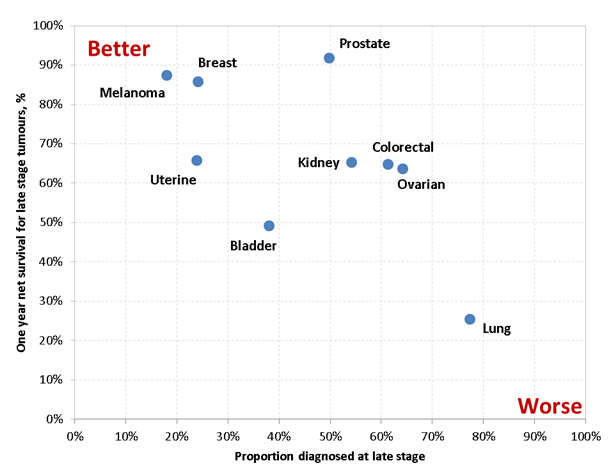
Another way of seeing this is to plot the proportion diagnosed at late stage against the one-year net survival (calculated as a weighted average) as shown below.
This clearly shows lung cancer as an outlier, and a commonly diagnosed one at that, with worse outcomes for the majority of patients.
Melanoma and breast cancer (also both common cancers) have both good outcomes and a majority of early stage diagnosed, while the other cancers examined here are intermediate between them.
Changing survival in cancer of unknown stage and what it might mean
The data quality is still improving, as can be seen by the falling proportion of cancers with an unknown stage over the last three years.
Where stage at diagnosis is known the changes in one-year survival are small, consistent with the slow change in overall cancer survival.
However, survival in the cancers with an unknown stage decreased significantly over the three year period 2012-14.
It is dropping for all cancers and is now consistently between the one-year survival for stage 3 and stage 4 cancers.
The reduction in survival implies that a higher fraction of unknown stage cancers are now in people who die rapidly after diagnosis, and are therefore likely have a later stage at diagnosis (although mortality could be due to other factors such as frailty or some other disease condition).
There will though always remain additional tumours that cannot be staged (such as sarcomas of the colorectum) or circumstances where it was clinically inappropriate to carry out a full staging process, perhaps due to patient frailty.
For these reasons we can never expect to reach a full 100% completeness for stage of cancer at diagnosis.
However, the enhanced collection of stage at diagnosis will allow us to observe and support positive trends in survival, give detailed feedback on initiatives to promote earlier diagnosis, and quantify the impact in stage specific survival due to changing clinical practice.