

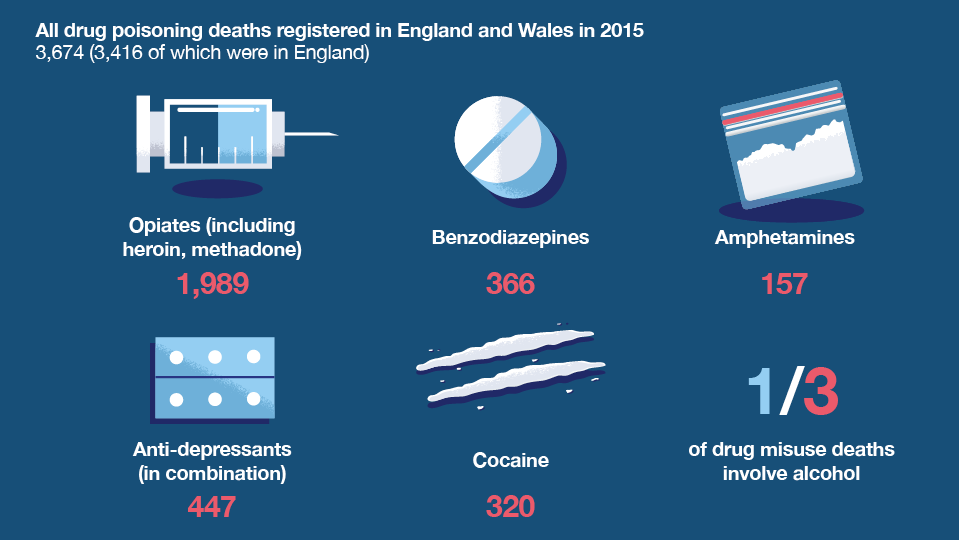
The latest edition of Health Matters highlights the record level of drug-related deaths in England.
This unquestionably warrants serious concern and efforts to improve the situation should be based on the best possible understanding of the problem including the trend itself.
One important observation made by the expert working group convened by Public Health England on drug-related deaths is that the sharpness of the increase seen in the number of deaths since 2012 is partly due to there having been a dip in the number of deaths registered between 2010 and 2012.
This means that while the number of drug misuse deaths registered in England in 2015 was 54% greater than in 2012, it was only 25% more than the previous peak of 2008.
It therefore perhaps makes sense to look back over a longer timeframe when trying to understand the trajectory.
Data on drug-related deaths in England (and Wales) began being reported in 1993.
Various factors have influenced the number of deaths recorded since then but there appears to be a ‘persistent background rise’.
This long-term trend is particularly evident in heroin/morphine-related deaths, which make up the majority of the total.

The factor most commonly suggested as contributing to recent increases in heroin-related deaths is the ageing cohort of heroin users, but such an explanation would seem a more comfortable fit for a long-term rise than for a sudden surge.
Even if we were to suppose a tipping point in the career length and/or the age of users after which mortality risk rockets, we would not expect so many heroin users to reach this point in such a short period of time given the variability in age and years of use among the cohort.
What caused this interruption in the long-term upward trend?
There is widely considered to have been a sudden, sharp reduction in heroin availability at the end of 2010 with heroin remaining relatively less available for a protracted period afterwards.
This period is commonly referred to as the ‘heroin drought’. The illicit nature of the heroin market means supply levels can’t be directly monitored and, because the resumption to pre-drought availability was more gradual than the initial reduction, the end of this period is less certain.
My team, the UK Focal Point on Drugs, reports to the EU’s drugs agency (EMCDDA) on behalf of the UK government and the devolved administrations.
We look broadly at the drug situation in the UK and monitor a range of indicators relating to users and health as well as to enforcement and supply.
We receive intelligence and data on drug markets from colleagues in the National Crime Agency. This includes data on the average purity of heroin seizures, including from samples of small quantity seizures, which serves as an indication of the purity of heroin encountered by users on the streets.
And we find purity primarily of interest because of the insight it gives us into the heroin market.
If demand doesn’t shift substantively from one year to the next, it can be presumed that the degree of adulteration in the supply chain will reflect (to a large extent) the amount of heroin that is available to spread among a relatively stable pool of users.
Using purity as a proxy indicator for availability, it appears that the heroin drought lasted throughout 2011 and 2012, with supply levels then increasing from 2013. This aligns fairly well with the pattern seen in heroin-related deaths.
There is no consensus regarding causes of the drought but we can be confident that it involved ‘upstream’ factors relating to international supply as it was experienced in several other European countries.
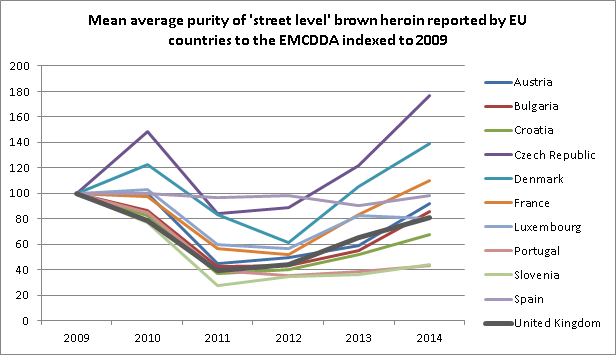
In line with the understanding of the drought as being an international phenomenon, average purity reported by other EU countries follows a similar pattern to that reported by the UK, supporting the validity of purity as an indicator of availability.
Of the member states reporting ‘street level’ purity of brown heroin to the EMCDDA continuously since 2009, almost all reported a fall between 2010 and 2011 with relatively low purity sustained to at least 2012.
Of course, the link between the pattern seen in average purity over time and the number of deaths is circumstantial and warrants investigation.
PHE is conducting analysis looking into whether the availability of heroin (measured through purity) impacts a range of indicators including deaths and we will be submitting this analysis for peer review.
Health Matters
Health Matters is a resource for professionals which brings together the latest data and evidence; makes the case for effective public health interventions and highlights tools and resources that can facilitate local or national action. Visit the Health Matters area of GOV.UK or sign up to receive the latest updates through our e-bulletin. If you found this blog helpful, please view other Health Matters blogs.