

In this blog we look at specialised commissioning and explain how it works and the role PHE plays.
What are specialised services?
Specialised services support people with a range of unusual and complex conditions. They often involve chemotherapy treatments provided to patients with cancers, genetic disorders such as cystic fibrosis , complex medical or surgical conditions such as kidney failure or complex mental health problems for example children and young people needing inpatient psychiatric care. Often they involve delivering cutting-edge care, such as proton beam therapy for brain tumours and are a catalyst for innovation and supporting pioneering clinical practice in the NHS.
How are specialised services commissioned?
Most NHS care is commissioned by local Clinical Commissioning Groups (CCGs). Specialised services are one of five areas which NHS England is centrally responsible for directly commissioning, alongside primary care, though this is usually delegated locally, some public health services, offender healthcare and some services for the armed forces.
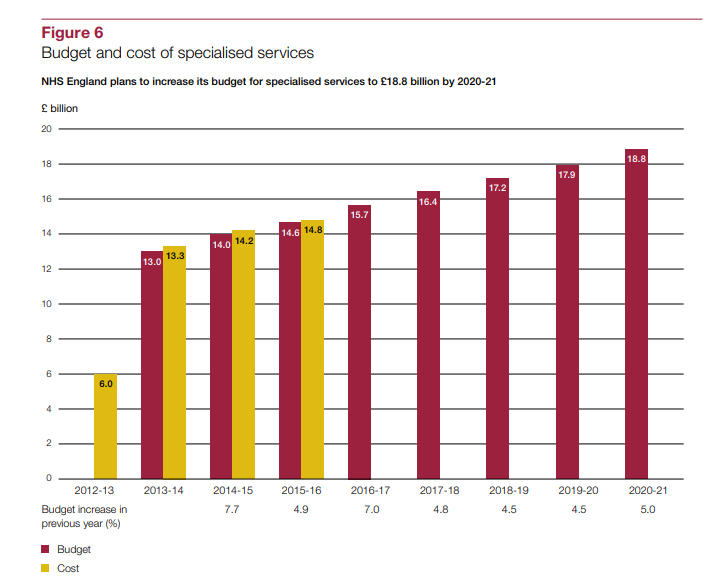
Figure is taken from the National Audit Office, full information can be found on page 21
How are PHE involved?
PHE provides expert advice to NHS England’s specialised service commissioning function which now has a budget of almost £17 billion – and has increased more rapidly than other parts of the NHS due to increasing demand for new drugs, interventions and other advances in medical technology.
How is PHE's advice provided?
We have staff members working in NHS offices nationally and in centres around the country, delivering PHE advice. Staff from across PHE, not necessarily working in NHS offices, also offer expert advice on many different areas, from health protection to health data.
The advice that PHE provides to specialised commissioning services aims to help the NHS get the best value from its resources in relation to the Five Year Forward View, which focuses on health outcomes, quality and efficiency.
What is the main aim of our contribution?
As we all know, funding is finite and should be spent on interventions which will have the greatest benefit on the health of the population, at the lowest cost.
Example of the benefits we see could be through cure rates or reduced levels of disability in childhood cancers, or through reduced levels of harm from new treatments.
The key question we are constantly asking when looking at specialised commissioning is always ‘how can we generate the most benefits with the most sensible funding?’
Proposals for new innovative treatments also often come through the route of specialised commissioning. This leads to small studies of treatments being carried out in expert centres, but this doesn’t always lead to the best value being found. An example here is an implantable electrical device to manage drug resistant epileptic fits.
The expert advice given by PHE makes a significant contribution to this agenda and helps NHS England to respond systematically to challenges in the use of its resources. The most important contribution we can make is to ensure investments are only made where there is strong evidence that a service is of value to the NHS.
Our focus is on ensuring resources are allocated to where greatest benefits can be achieved, recognising that demand always outstrips resources available.
Examples of PHES contribution:
A particular contribution from PHE has been to provide “deep dive” reports on five of the top spend areas within specialised commissioning involving up to £1 billion (such as Neonatal Intensive Care (NICU), to identify how improvements elsewhere in a pathway could help to reduce demand.
In the case of NICU the most important change identified by this work was the importance that reducing maternal smoking could have on demand for these services (through reducing low birthweight and premature labour) which impacts on need for neonatal care.
Another report on renal dialysis highlighted the impact that improved control of blood pressure and diabetes could have on slowing the demand and need for treatment of renal failure. The move to integrated care systems and pooling of budgets in local areas as envisaged by the current integrated care system could potentially allow work such as the “deep dive” reports to inform service transformation and the allocation of resources.
Examples of other contributions
Advice supporting the development of a systematic and structured decision support process (including consistent approach to evidence used to make decisions)
Advice to Individual Funding Requests – these are high risk decisions frequently subject to public scrutiny through judicial review relating to funding for services which are not routinely commissioned and for which often evidence is limited or lacking.
Disinvestment from existing services – Current considerations are ongoing about how to construct and implement a fair and feasible process to disinvestment in specialised services.
Honing down the right questions to support evidence based policy making – what exactly is the evidence question PICOS
Data analysis – PHE is the holder of significant population healthcare information e.g. cancer chemotherapy use and in general by using our information source we can help advise on service configurations
You can learn more about specialised services and watch an explainer animation via NHS England.